This is the most common of the indolent lymphomas and accounts for about 70% of them, and about 22% of all lymphomas in North America and Europe. At the bottom of this page is an explanation of where the name follicular comes from and what it looks like under the microscope.
Follicular lymphoma is divided into 3 grades. Grade 1, 2 or 3. However Grade 3 is somewhat blurry because it can appear to be the indolent form of follicular lymphoma or it can appear to be the more aggressive form. You can read more about Grade 3 fNHL in the Additional Topics section further down this page. The grade refers to the number of large cells that appear under the microscope. Large cells tend to behave a bit more aggressively than small cells. Although more large cells appear in Grade 2, it is for all intents and purposes considered the same as Grade 1 from a prognosis and treatment point of view. See more information below about grade 3 follicular. If you are confused about the difference between grade and stage you are not alone. Here are links to the two definitions.
The Follicular Lymphoma International Prognostic Index (FLIPI) is a tool that can be used to estimate the prognosis and the survival odds at 5 and 10 years.
Follicular lymphoma is a slow growing type of NHL which responds very well to treatment, but can rarely be cured, except when it is found in stage I. In those cases sometimes radiation is able to cure the fNHL if it is truly localized to a single location. (11) Despite the fact that it cannot be cured, the prognosis is generally very good and the median survival is about 8-15 years according to the NCI. However the Stanford University school of medicine has authored a long term study showing that since 1960 the median survival has increased from just 11 years in that decade, to over 18 years in the pre-Rituximab era, and in the current Rituximab era the median has not been reached after about 12 years of follow up. (1) This study was published in June 2013. Presumably once enough years have passed since Rituximab was introduced (1997) we will have updated data. Maybe we will find overall survival is over 20 years. (2)
Age also plays an important role in the prognosis. Data from the 2011 ASH convention shows that the median cause specific survival for patients under the age of 40 is 24 years. (3) Cause specific survival refers to the people who did, or did not die of their follicular lymphoma as opposed to other causes of death. This is quite different from overall survival which simply refers to the number of people who are still alive, regardless of their cause of death. Quite simply put, those over 60 are obviously at higher risk of dying of "something" than those under 40. In fact one study showed that after a median of 10 years only 35% of patients had died, and only 13% died from the lymphoma. (5)
How you respond to your initial therapy is also a significant prognostic indicator. An Italian study, from the 2015 ASH abstracts shows that the median survival for patients who were responsive to their primary treatment have a median survival of 32.6 years. (12) That study covered the years from 1976-2012 and included 597 patients.
One of the primary concerns for any patient with follicular or other indolent lymphoma is transformation to a more aggressive lymphoma such as diffuse large B-cell lymphoma. Click the link below to read more about transformation.
Information about Transformation
In many cases treatment may be deferred and a watch and wait approach is appropriate. Studies have consistently shown that there is no survival benefit to treating immediately versus waiting until treatment is necessary. (14) (4) (13) This holds true, even for advanced stage patients. (5) For some patients the idea of having cancer and doing nothing about it can be a difficult concept to accept. They may prefer to initiate treatment immediately even though it provides no survival benefit. But the act of “doing something” is emotionally more appealing.
What confuses the issue however is the availability of low toxicity treatment like Rituxan or radioimmunotherapy. With their low toxicity and high efficacy it might be time to abandon watch and wait in favour of these therapies. It is known that they will delay the time until more aggressive chemotherapy is required. Treatment with Rituxan alone for newly diagnosed follicular lymphoma that is asymptomatic has been shown to be highly effective and may be an excellent choice for those patients who are not comfortable with watch and wait. (6) Rituxan followed by Rituxan maintenance has also been shown to be effective at delaying the time until more toxic chemotherapy is needed, but it does not improve the overall survival. (7) When deciding whether watch and wait, or Rituxan therapy should be used the patient must weigh the cost and inconvenience of going for therapy every few months, versus delaying the need for chemotherapy.
Some of the factors that may indicate the need for treatment include:
When treatment is initiated there are many options to choose from. There are no right or wrong choices and patient preference often plays a role. Some prefer the mildest effective treatment to preserve lifestyle and healthy living, others prefer more aggressive upfront treatment for peace of mind and the feeling of eradicating the disease. Both approaches have merit. Listed here are options from mild to more aggressive.
Oral Chlorambucil is a very effective treatment though it has fallen out of favour. Lack of profit for the prescription drug is a motivating factor. Nevertheless this alkyating agent is highly effective in fNHL, very convenient, and has an excellent side effect profile.
As discussed above single agent Rituxan is a good choice. Rituxan is a monoclonal antibody therapy and not chemotherapy. You can read more about monoclonal antibodies by clicking here. Where Rituxan really shines though is when combined with chemotherapy. In that setting there appears to be a highly synergistic effect.
Next would be combination chemotherapy such as:
Historically CVP+Rituxan and R-CHOP have been the most widely used treatments when therapy is required. CVP is highly effective and reserves the option of using the anthracycline (the Doxorubicin) in CHOP for later if required.
However recent data shows that Bendamustine+Rituxan may be superior to R -CHOP (8) (9) with lower rates of toxicity. Although Bendamustine has been around for many decades in Europe, it was only recently (around 2007) started to be used in North America.
There still remain some unanswered questions about Bendamustine+Rituxan. The first question is with respect to secondary cancers years down the road. Most chemotherapy regimens are known to significantly increase the risk of secondary cancers 10-15-20 years down the road. It will take many years before we know if Bendamustine makes that risk higher, or lower than other treatments.
The other unanswered question is whether or not using Bendamustine will reduce the effectiveness of future therapies when they are required. This too is a question that will take many years to answer.
The Cancer Network has a thorough review of the management of follicular lymphoma in the upfront and relapse setting. Although you need to create an account with the Cancer Network, it is free. This review is a comprehensive review of current practice throughout the world, and in clinical trials. It reviews the commonly used treatments, the outcomes of those treatments, the patient characteristics and future directions. This is a must read.
Management of Follicular Lymphoma in the Up-Front and Relapsed Settings from the Cancer Network
Next are two articles from two prominent experts in lymphoma. In each article they discuss the current approaches to treatment and management of follicular lymphoma. What is most notable is that even in this modern era there is still no once size fits all approach. With many treatment options that are highly effective, the decision often becomes a consensus discussion between the patient and their doctor.
Bruce D. Cheson, MD: How we Manage Follicular Lymphoma
Therapy of newly diagnosed follicular lymphoma
After initial treatment has been completed it is is becoming increasingly common to consolidate that treatment by including maintenance Rituxan or consolidation with radioimmunotherapy. Consolidation therapy has been shown quite conclusively to prolong progression free survival. Whether it improves overall survival is still not clear, but it is hope that this proves true. The USA National Comprehensive Cancer Network has now included consolidation as a Category 1 level of evidence and consensus as frontline treatment for follicular lymphoma. This is their highest category indicating that there is ample evidence to support their recommendation and there is uniform consensus from their panel of experts. It will not be surprising to see this approach used for other types of indolent lymphoma as well.
Vaccines are becoming increasingly investigated to maintain remissions. It just makes sense that if you can achieve remission with treatment, then a vaccine can prevent it from coming back. Visit our vaccines page for details about many of the vaccine options under investigation. A study from 2011 looks at the possibility of using a vaccine instead of maintenance Rituxan to maintain a remission. This appears to be a promising option but it is still too early to know if it can replace maintenance Rituxan. (10)
What about Stem Cell Transplants? Should they be used for follicular lymphoma? This has long been a controversial issue with many differing opinions. In 2013 the European group for Blood and Marrow Transplantation did an in-depth study and analysis with many expert haematologists to come up with a recommendation for the proper time to use SCT for fNHL.
Simply put they do not recommend SCT as first line therapy even for high risk patients. They do recommend it for patients in first relapse who had a short remission. They also have additional recommendations. Read the study below.
Below is a link to an experts review of the above study. Sometimes a non technical review helps put things in better perspective.
Transplantation in follicular lymphoma: not “yes or no” but “whom and when”
Here is another review from 2016 of all the data concerning transplanting indolent lymphoma in general.
Here is some additional information on this very controversial topic from the Journal of Clinical Oncology. It is a very provocative discussion and shown here in 3 parts. The first part is a peer review of the original study. The second part is the original authors reply to that. Finally the original study that they are discussing.
Should We Transplant Indolent Lymphoma?
Below are some additional studies that examine the role of stem cell transplants for follicular lymphoma.
The following study looks at the results of using SCT versus more traditional chemotherapy for follicular lymphoma patients in their first relapse. The SCT arm has dramatically improved results.
Here is a study that looks at the long term outlook for people who have had a relapse after an SCT. It also reports on the risk of relapse after SCT (less than 50% relapse rate.)
A 2010 study examines the role of mini-allogeneic transplants using in-vivo purging and Donor Leucocyte Infusions. The patients in this study had been heavily pre-treated with a median of 4 prior therapies including some patients who had an autologous SCT previously.
They first deplete the patients T-cells using Fludarabine, and Alemtuzumab to help promote full donor chimerism after the transplant. They hypothesize that a significant percentage of their patients are cured using this approach.
Perhaps this is not as true as it has been in the past. Below are some recent studies which show how long term survival is becoming more common for follicular lymphoma.
From the Cancer Network (free membership is required) an expert article that discusses several types of lymphoma. But for follicular lymphoma they examine the data that shows the median survival 25 years ago was only 5-10 years, and now it is approaching 20. This means that most people with fNHL are not likely to die from the lymphoma.
New Treatment Options Have Changed the Survival of Patients With Follicular Lymphoma
The following retrospective study looks at the dramatic improvement in survival over the past 3 decades, with the Rituxan era showing a huge improvement of 5 year survival from 80% in the 1970's to 91% in the Rituxan era.
Patterns of survival of follicular lymphomas at a single institution through three decades
Following is a review of the potential curability of advanced fNHL by Fernando Cabanillas from MDA
Curability of Advanced Indolent or Low-Grade Follicular Lymphomas: Time for a New Paradigm?
A response from another expert (Ian Edwin Haines)
Should the Paradigm Shift for Low-Grade Follicular Non-Hodgkin Lymphoma Be Toward Less Therapy?
And finally a response from the original author Fernando Cabanillas
Here is an excellent Continuing Medical Education article (CME) which discusses whether or not radioimmunotherapy offers the chance to cure follicular NHL. (Paid subscription required)
Radiolabeled and Native Antibodies and the Prospect of Cure of Follicular Lymphoma
Next is a 2012 study that has over 11 years follow-up. In this study they used a non-myeloablative allogeneic stem cell transplant to achieve a 78% progression free survival at a median of 11 years follow-up. That is very impressive.
In 1998 a study was started which examined using extended Rituximab to see how it would affect survival of patients with fNHL. The first results from that study were published in Blood in 2004 and looked very promising. The results were updated at the ASCO convention in 2009 and continued to show a benefit of extended Rituximab. Here are the results.
Medscape has an excellent article which discusses the above study and puts it into perspective and how a cure may actually be achievable. Medscape requires a membership to view its articles, but membership is free and takes only a minute to setup.
ASCO 2009: Prolonged Rituximab Extends Remission in Follicular Lymphoma
Below is a detailed description of the pathology of follicular lymphoma. It may help to give a better understanding of exactly how it occurs and some of the challenges understanding it.
One of the key points to remember about lymphoma is that there is no single cause. You cannot point at any single risk factor such as pesticide exposure and say, "THAT" caused my lymphoma. It takes multiple mutations to the cell before it becomes cancer. As a case in point, the t(14:18) chromosomal mutation is the hallmark of follicular lymphoma. Virtually all follicular lymphoma patients have that mutation. But surprisingly so do many of the healthy population. Some of those healthy people go on to develop follicular lymphoma and others do not. Here are some detailed articles on that topic and what else is necessary to develop fNHL.
Nature and importance of follicular lymphoma precursors
Next is a study about the t(14:18) mutation.
Human t(14;18)positive germinal center B cells: a new step in follicular lymphoma pathogenesis?
Here is a peer review that discusses what the above link means.
Molecular pathogenesis of follicular lymphoma
This type of follicular lymphoma has commonly been associated with a worse overall survival rate. But this is highly controversial, and different studies show different results. The follow study reveals that dividing grade 3 into 3a (similar to grade 1 & 2) versus grade 3b (similar to diffuse large B-cell) is not exact enough. It must be divided into grade 3 with less than 50% diffuse component, versus grade 3 having more than 50% diffuse component. Grade 3 with <50% has an outcome very similar to grade 1 & 2.
Here is more information about low grade and grade 3 fNHL
A very recent study looks at the genetic features of Grade 3 follicular lymphoma. While it does not make ground breaking conclusions it does find additional information about the features of this type of NHL. It finds that some grade 3B follicular lymphoma's are purely follicular, while others are really DLBC with a grade 3B follicular component. As always however, diagnosing this is an advanced art, and requires detailed molecular and genetic testing which is not routinely done on every follicular patient.
Here is a peer review of the above article by another lymphoma specialist.
Follicular lymphoma grade 3B: is it a real disease?
Follicular lymphoma: evolving therapeutic strategies
Medscape article about follicular lymphoma
NCI information about indolent lymphomas
The tumour microenvironment is currently a very hot area of research. This is referring to the role the healthy cells in the tumour behaviour and prognosis of follicular NHL.
Click here for more detailed information about the microenvironment
The name of this lymphoma derives from the location and behaviour of the cancerous cells. They usually originate in the lymphoid follicles, but more important is that they grow in a follicular pattern. This means that the cells tend to clump together or "stick" together.
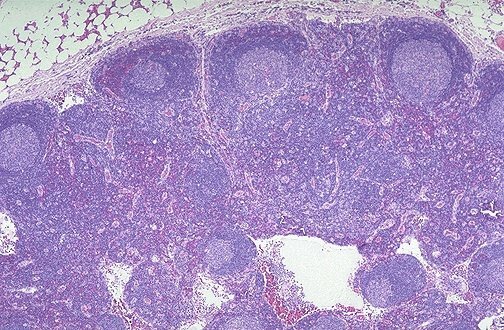
Above is an image of a normal lymph node slice at a medium magnification. Notice how it has those round "follicles" around the outer top edge. They are the pale purple circles you see. That is what a normal lymph node should have. For a drawing of the same thing click here:

Here is slide of a lymph node with follicular lymphoma. Notice how many more of those follicles there are! And notice how tightly packed they are throughout the node, rather than just at the outer edge.
While follicular lymphomas very often form outside of the lymph nodes, it is this follicular pattern of growth that gives it its name. (past classification systems called it nodular)